Hairline distortion after face lift procedures can be a problem, especially in the sideburn, temporal, and retroauricular areas. Although the retroauricular hairline is less exposed than the temporal hairline, it is still aesthetically important; its displacement during a face lift can result in a significant and noticeable deformity. Retroauricular hairline deformity usually appears as a 90-degree angle of hairless skin that can be described as a “step” design or upward hairline displacement. Patients are frequently stressed and self-conscious about the appearance of their hairline in such cases, and women with retroauricular hairline distortion may refrain from gathering their hair up in a style that exposes the neck.
This problem can be prevented with the use of a pre-hairline incision, slightly into the hairline, but when it does occur, it can be corrected with a simple, safe office procedure. Local anesthesia alone may be used; for increased patient comfort, I recommend intravenous sedation and local anesthesia.
Headington1 studied the transverse microscopy of the scalp and found that hair grows in follicular units – that is, in groups of 1, 2, 3, or 4 hairs, with each group containing an independent neurovascular bundle, sebaceous glands, and piloerectile muscle, all surrounded by a fine circumferential sheath of collagen. These units appear, to some degree, to be true physiologic entities, so that maintaining them as intact as possible improves hair survival and ultimate hair growth.
The technique I present is very similar to my technique for correcting postrhytidectomy “lost” sideburn.2-3 Here, I apply it to the retroauricular area, using micrografts (1 or 2 hair follicular units) and minigrafts (3 or 4 hair follicular units) to correct the retroauricular hairline step deformity. Such small grafts survive even on scar tissue, including burn scars.4 I treated 15 women with retroauricular hairline step deformity, ranging from 42 to 65 years, between January 1996 and January 2002.
Technique
With the patient supine, and usually under mild sedation with midazolam hydrochloride and fentanyl, I turn the patient’s head to the left and infiltrate 0.5% Marcaine (Abbott Laboratories, N. Chicago, IL) with epinephrine into the donor site, which is a horizontal ellipse of scalp from the occipital area, generally 3 by 0.5 cm, depending on the number of grafts planned. I carry out dissection, using 3.5 power magnifying loupes or under a microscope at a magnification of 10x, generating 150 to 300 or more follicular unit micrografts (1 or 2 hairs) and minigrafts (3 or 4 hairs), depending on the degree of the deformity. I make sure to use very small grafts, as with male-pattern baldness, to avoid the “hair plug” look.
I perform the harvest and graft dissection using no.10 Bard-Parker blades (Becton Dickinson, Canaan, CT). After locally anesthetizing the recipient sites with Marcaine solution, I use 22.5 Sharpoint blades (Sharpoint, Reading, PA) and jeweler’s forcepts to insert the grafts. I insert the blade at the same angle and in the same direction I want the hair to grow, usually a very acute angle, 30 degrees or less. I make a slit until the grafts are densely packed; they are separated by about 1.5 mm.
Results
Significant improvement is usually evident in 3 to 4 months. You can see the final result after 8 to 10 months. Patients are usually very satisfied with 1 session; however, if the patient desires greater density, a second session can be arranged. Of the 15 patients in this series, 13 were satisfied with 1 session and 2 patients underwent 2 sessions. No patients experienced infection, keloid scars, inclusion cysts, or any significant problem.
Although other techniques such as scalp flaps and tissue expansion can be used to correct this deformity, all leave a scar in front of the new hairline.
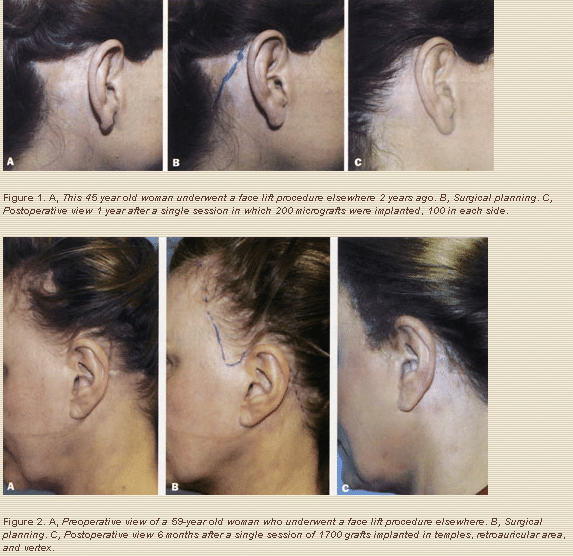
The safety, simplicity, and natural appearance achieved with the use of follicular unit micorgrafts and minigrafts make this technique, without a doubt, a better way to correct such deformity. Furthermore, this technique leaves no scars in front of the new hairline (Figures 1 and 2).
References
1. Headington, JT. Transverse microscopic anatomy of the human scalp. Arch Dermatol 1984; 120:449-456.
2. Barrera A. The use of micrografts and minigrafts for the correction of the postrhytidectomy lost sideburn. Plast Reconstr Surg 1998;102:2237-2240.
3. Barrera A. Hair grafting tips and techniques. Perspect Plast Surg 2001;15:147.
4. Barrera A. The use of micrografts and minigrafts for te treatment of burn alopecia. Plast Reconstr Surg 1999;103:581.
Alfonso Barrera, M.D.
West Houston Plastic Surgery Clinic, P.A.
915 Gessner Rd., Suite 825
Houston, TX 77024
