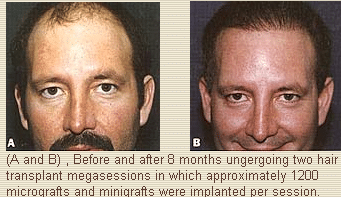
Exciting advances in hair transplantation have been introduced in recent years, particularly the use of a large number of micrografts (containing only one or two hairs) and minigrafts (containing three or four hairs) in a single hair transplantation megasession. A megasession consists of the placement of more than 1000 grafts in a single session.
This study includes data from 105 consecutive micrograft and minigraft megasessions performed between March 1994 and August 1996 in 100 patients, with a follow-up of 5 months to 33 months. The patients included 96 men and four women whose ages ranged from 21 to 67 years, with an average age of 42 years.
In this procedure a horizontal ellipse of scalp harvested from the donor’s occipital area is used to make grafts under 3.5 loupe magnification. The grafts are inserted through slits in the recipient area, and the donor site is closed primarily. All of the procedures were done at my office surgical suite with the patients under intravenous sedation and local anesthesia. This procedure was found to be safe and predictable. The only complications encountered were a hypertrophic donor site scar in one patient (I %) and self resolving ingrown hairs (cysts) in nine patients (9%). Ninety-seven patients (97%) were satisfied with the results obtained after one session. Three patients (3%) who were dissatisfied with the results after one session were pleased with the results obtained after a second procedure.
For the most part the various procedures available over the years to treat male pattern baldness have tended to require too many sessions and leave too much scarring, and have yielded an unnatural result. In recent years the use of micrografts was introduced in an effort to obtain a more natural appearance in the front hairline after use of traditional hair transplantation techniques. (1-15)Micrografts were able to camouflage the front hairline by providing a transition zone of fine hairs before the wall of hair that begins abruptly with use of flaps; micrografts were also able to camouflage the “corn row” appearance of conventional round plugs. (16-18)More recently the use of a large number of micrografts and minigrafts to cover an entire area of baldness has opened up new possibilities for the treatment of male pattern baldness. Use of these grafts makes it possible to complete a hair transplantation in just one or two sessions without visible scarring and provides a natural result over the entire head.(19-21)
Between March 1994 and August 1996 I performed micrograft and minigraft megasessions in 113 patients. Thirteen patients were eliminated from this study because they were either lost to follow-up or had not been monitored for a long enough period. I performed 105 megasessions in the remaining 100 patients, all of whom were followed up closely from between 5 months to 33 months. Ninety-five patients underwent a single megasession, and five patients underwent two megasessions. The number of micrografts and minigrafts implanted in each patient per megasession ranged from 1000 to 2500. The majority of patients undergoing hair transplantation today receive approximately 2000 grafts.
As I have become more comfortable with this technique I have occasionally performed other aesthetic procedures at the same time as the hair transplantation procedure. These aesthetic procedures have included primarily upper eyelid blepharoplasty, upper and lower lid blepharoplasty, rhinoplasty, otoplasty, and liposuction. In addition, when performing a face lift I sometimes use the pieces of scalp that are normally discarded to make micrografts and minigrafts and insert them in areas where these grafts are needed.
Technique
I use a four-person surgical team for all hair transplantation cases. The patient, who is in the supine position, is sedated with intravenous Versed (midazolam) and Sublimaze (fentanyl citrate). For a local anesthetic I use Marcaine (bupivacaine) 0.5% with epinephrine 1:200,000 (usually a total of 40 ml) to block the supraorbital, supratrochlear, and occipital nerves, Subsequently tumescence is induced in both the donor and recipient areas with use of 0.5% Xylocaine (lidocaine) with epinephrine 1:200,000. (Usually a total of 150 ml is used throughout the procedure.) With a No. 10 scalpel blade a horizontal ellipse of scalp measuring 10 to 25 cm long by 1.5 to 2 cm wide (depending on the number of grafts to be made and the thickness of the hair in the donor area) is harvested from the occipital area (Figure 1, A). The area is subsequently undermined and closed primarily.
With the patient in the supine position and his or her head turned to one side, I harvest half of the ellipse. As I am closing the donor site my assistants start making grafts from the harvested section of scalp (Figure 1, B and Q. The patient’s head is then turned in the opposite direction so I can harvest the second half of the ellipse. Several interrupted sutures and a running suture of 3 “0” Prolene close the incision.
Personna prep blades or No. 22 blades are used to cut the grafts, which are then inserted through small slits made with a No. 65 Beaver miniblade or a Feather 11 Personna blade (Figure 1, D and E). The micrografts are inserted at the very front and the minigrafts are inserted posterior to the frontal hairline. I personally insert all the grafts to ensure uniformity. The procedure takes 4 to 6 hours, depending on the number of grafts. The bandage is removed 48 hours after the surgery, at which time the patient is allowed to shampoo his or her hair daily.
Results
All patients were closely followed up and evaluated for evidence of infection, hematoma, dehiscence of the donor site, deforming scars, ingrown hairs or inclusion cysts, permanent numbness of the occipital area, poor hair growth, and any other potential complication. Only two types of complications were encountered. Nine patients (9%) had self-resolving ingrown hairs and cysts. These ingrown hairs and cysts became evident at 3 to 4 months after the surgery, matured, and erupted spontaneously, yet they still resulted in hair growth. The incidence of this complication has been reduced to almost 0% by inserting the grafts more superficially. Heating may be expedited by incision and drainage with a needle. The other complication occurred in one patient (I%), a black man, in whom a hypertrophic scar developed at the donor site. Fortunately the appearance of the scar improved following the use of Kenalog’ (triamsinolone). Individuals with dark skin are more prone to have hypertrophic scars.
To evaluate patient satisfaction with the results, all of the patients were interviewed personally and photographed by me and my staff. Follow-up ranged from 5 months to 33 months. As with any other procedure, the patients were selected carefully and particular emphasis was placed on the need for realistic expectations. It is essential that patients have a clear understanding of the density limitation of the procedure-namely, that it involves a redistribution of their existing hair.
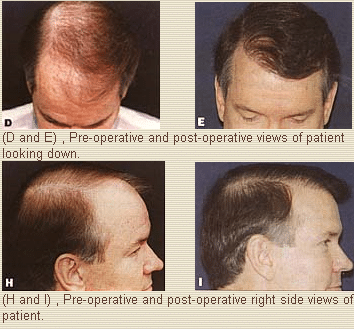
The rate of patient satisfaction after a single micrograft and minigraft megasession (Figure 2) was 97% (97/100). Only three patients (3% were dissatisfied after a single megasession because the hair growth was not as dense as expected. However, these patients were pleased with the result after undergoing a second megasession. Judging from the uniformity of the hair growth pattern that I observed after these procedures, it appears that successful hair growth results from at least 90% to 95% of the grafts. The fact that micrografts and minigrafts are so small and are inserted into slits seems to enable them to survive even in the precarious environment of scarred recipient tissue. Naturally the per-graft yield is lower in cases of severe scarring. I have observed this lower yield in patients who had prior scalp reductions, scalp flaps, and especially in those who had multiple sessions of traditional round, large hair plugs. If the scarring is not very severe I have noted that approximately 80% to 85% of the grafts (on scarred tissue) result in growing hair.
Although transplanted hair begins to grow immediately after a micrograft and minigraft megasession, a great deal of it sheds in about 3 to 4 weeks, when it goes into telogen. The patient needs to be reassured that most of the hair grows back in 3 to 4 months as it goes into anagen. By the fifth to sixth month the hair begins to look attractive; however, it takes about a year before the final result is achieved.
Conclusions
I have found that the described hair transplantation procedure is safe, predictable, and yields a high level of patient satisfaction. Most patients are encouraged by the fact that this technique can produce a result that looks natural despite the density limitation and can be performed in only one or two sessions.
A distance of approximately 1.5 rnm must be maintained between grafts for optimal graft take and subsequent hair growth. This obviously becomes a density limitation for a given megasession. Another megasession in which grafts are inserted between those placed in a previous procedure may be repeated 8 months to a year later to obtain greater density. Micrograft and minigraft megasessions can be repeated as long as sufficient donor site density exists. In my opinion, the maximum density feasible with this technique is achieved after two to three megasessions (Figure 3). 1 also believe that even those patients who have only one megasession and never return for another hair grafting session can obtain significant improvement and a natural appearance.
References
1. Orentreich N. Autografts in alopecia and other selected dermatological conditions. Ann N Y Acad Sci 1959;83:463.
2. Stough DB. Punch scalp autografts for bald spots. Plast Reconstr Surg 1968;42:450.
3. Vallis CP. Hair transplantation for male pattern baldness. Surg Clin North Am 1971;51:519.
4. Juri J. Use of parieto-occipital flaps in the surgical treatment of baldness. Plast Reconstr Surg 1975;55:456.
5. Elliott RA, Lateral scalp flaps for instant results in male pattern baldness. Plast Reconstr Surg 1977;60:699.
6. Mayer TG, Fleming RW. Short flaps: thin use and abuse in the treatment of male pattern baldness. Ann Plast Surg 1982;8:296.
7. Blarchard G, Blanchard B. Obliteration of alopecia by hair lifting: a new concept and technique. J Natl Med Assoc 1977;69:639. B. Alt TH. Scalp reduction as an adjunct to hair transplantation: review of relevant literature, presentation of an improved technique. J Dermatol Surg Oncol 1980;6:1011.
9. Unger MG. The modified major scalp reduction. J Dermatol Surg Oncol 1988;14:80.
10. Brandy DA. Point: extensive scalp-lifting. J Dermatol Surg Oncol 1988;14:1420.
11. Manders EK, Au VK, Wong RKM. Scalp expansion for male pattern baldness. Clin Plast Surg 1987;14;469.
12. Adson MD, Anderson RD, Argenta LC. Scalp expansion in the treatment of male pattern baldness. Plast Reconstr Surg 1987;79:906.
13. Anderson RD. Expansion-assisted treatment of male pattern baldness. Clin Plast Surg 1993;7:477.
14. Anderson RD. The expanded “BAT” flap for the treatment of male pattern baldness. Ann Plast Surg 1993;31:385.
15. Frechet P. Scalp extension. J Dermatol Surg Oncol 1993;19:616.
16, Marritt E. Transplantation of single hairs from the scalp as eyelashes. J Dermatol Surg Oncol 1980;6:4.
17. Nordstrom REA. “Micrografts” for improvement of the frontal hairline after hair transplant. Aesthet Plast Surg 1981;5:97.
18. Marritt E. Single-hair transplantation for hairline refinement: a practical solution. J Dermatol Surg Oncol 1984;10:12.
19. Uebel CO. A new method for pattern baldness surgery. Presented at Jornada Carioca C~rurgia Plastica; August 1986; Rio cle Janeiro, Brazil.
20. Uebel CO. Micro and minigrafts: a new approach to baldness surgery. Ann Plast Surg 1991;27:476.
21. Barrera A. Micro and minigraft megasession hair transplantation: results after a single session. Presented at the Sixty-fifth Annual Scientific Meeting of the American Society of Plastic and Reconstructive Surgeons, Plastic Surgery Educational Foundation, and American Society of Maxillofacial Surgery; November 1996; Dallas, TX.
Alfonso Barrera, M.D.
West Houston Plastic Surgery Clinic, P.A.
915 Gessner Rd., Suite 825
Houston, TX 77024
