Surgeons who perform rhytidectomy (face lift procedures) know that there are times when the upward displacement of the sideburn is greater than desired. The sideburn and temporal hairline are aesthetically essential features of the face. When there is a mild loss, it may go unnoticed; however, in some cases, it can be more severe, especially in secondary or tertiary procedures, resulting in a tell-tale deformity unique to rhytidectomy. These patients have great difficulty in styling their hair, and they lose the freedom to style their hair upwards or back. To correct this deformity, the hair must be restored. Punch grafts, various scalp flaps, free scalp flaps, and scalp tissue expansion have been described as ways of doing so.
In an effort to obtain a result that is as natural as possible with a minimum of scarring and down time, I use micrografts (grafts with one or two hairs) and minigrafts (grafts with three to four hairs). The technique is basically the same as the one previously described for the treatment of male-pattern baldness; the main difference is the direction and ang-ulation of the graft insertion, which provides a more natural sideburn and temporal hairline.
Technique
In our office surgical suite, with the patient in the supine position, intravenous sedation is administered with midazolam and fentanyl. Nerve blocks to the occipital and auriculotcmporal nerves are performed with 0.5 percent bupivacaine and epinephrine 1:200,000 (about 30 cc). Then, tumescent infiltration with 0.25% lidocaine 1:200,000 is done in both the donor and the recipient sites as needed (about 60 cc).
A horizontal ellipse is harvested from the occipital area. It usually measures 4 to 5 X I to 1.5 cm, depending on the number of grafts we expect to be required. The donor site is closed primarily with a single layer of simple running 3-0 Prolene sutures. The grafts are then prepared with Personna preparation blades (American Safety Razor Company, Verona, Va.) and no. 22 blades. The proposed new anterior temporal hairline and sideburn are marked in ink, and we then insert the micrografts and minigrafts as close as possible, about 1.5 mm, to each other.
Slits are created in the areas of hair loss with a Feather no. I I Personna blade or a 65 Beaver miniblade. The blade must be inserted at a very acute downward angle in the same direction as a natural sideburn and the anterior temporal hair to obtain hair that will grow in that direction. There is no need for sutures in the recipient site. As the fibrinogen turns into fibrin, the grafts become secure enough.
For the first 48 hours, a dressing is applied consisting of adaptic, kerlix and a 3-inch elastic bandage. After that, the patient is allowed to shampoo gently. We prescribe 500 Ing of cephalexin to be taken orally, four times a day, and acetaminophen with codeine for the first few davs. The donor site sutures are removed 7 to 10 days postoperatively. It takes 10 months to I year for the final result.
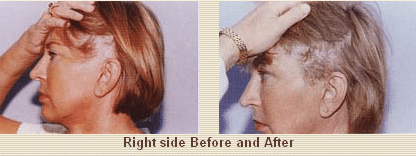
Clinical Cases
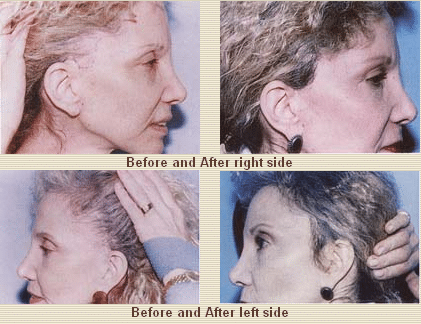
Case 1
Discussion
The loss of the sideburn after a face lift procedure is a topic not frequently discussed. When mild, it often goes unnoticed; but when it is more severe, the patient is usually told to simply style the hair carefully to hide the deformity. Several other techniques to correct the problem have been described. I believe that using micrografts and minigrafts is a simple and safe solution that can completely correct this deformity in a single session, as demonstrated.
I have also noticed that when the donor hair is harvested from the nape of the neck to harvest finer hairs, there is a greater tendency to develop hypertrophic scarring of the donor site. I prefer to harvest from a more cephalic location in the occipital area, as in cases of male-pattern baldness, where such a tendency is almost totally eliminated. I have had a high level of patient satisfaction. If desired, as in the treatment of male-pattern baldness, the procedure may be repeated for additional density.
Conclusions
The use of micrografts and minigrafts for the correction of the lost sideburn after rhytidectomy is safe and effective in obtaining an excellent and natural result in a single session.
Summary
A tell-tale and unsightly deformity that can result from a rhytidectomy is the loss of the sideburn. As redundant skin is lifted, the hairless skin of the cheek may be advanced into the sideburn area. Several techniques have been described for sideburn reconstruction, mainly punch grafts and various scalp flaps.
I use micrografts and minigrafts to effectively correct this deformity in a single session, under local anesthesia and mild intravenous sedation. I use basically the same technique previously described for the treatment of male-pattern baldness, with the direction of graft insertion being at a very acute angle to obtain the growth of hair in a natural downward direction. I found the procedure safe and predictable, and the patients treated were very satisfied with the aesthetically pleasing and natural result.
Alfonso Barrera, M.D.
West Houston Plastic Surgery Clinic, P.A.
915 Gessner Rd., Suite 825
Houston, TX 77024
