Background: Great advances have taken place in recent years in hair transplantation for both aesthetic and reconstructive purposes. However, there are still cases in which results do not appear entirely natural. This may be a result of slight clumps caused by grafts that contain too many follicles, scarring, and hair lines that are too straight, too low, too thin, or otherwise artificial. Furthermore, too many surgical sessions (4, 5, or more) are often required for an aesthetically pleasing result.
Objective: A procedure for achieving natural and aesthetically pleasing hair restoration in 1 or 2 sessions through the use of large numbers of follicular micrografts and minigrafts is described.
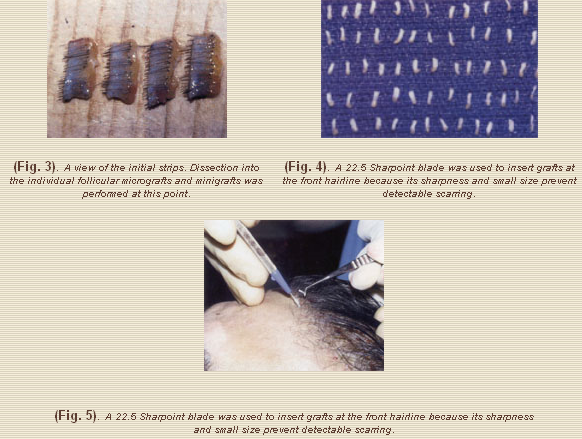
Methods: Between March 1994 and March 2002, more than 400 consecutive patients underwent hair restoration with 2000 to 2500 micrografts and minigrafts. A horizontal ellipse of skin was harvested from the occipital area and dissected into 2-mm strips by the surgeon. The strips were further dissected into individual micrografts or minigrafts by surgical technicians. The grafts were inserted with the use of a technique in which scalp slits were made by the surgeon using a 22.5 Sharpoint (Surgical Specialties Corp, Reading, PA) blade and an assistant immediately inserted the graft by sliding it along the side of the blade. This process was repeated until all grafts were inserted and densely packed, about 1.5 mm apart.
Results: Satisfactory results with few complications were obtained predictably in 1 session. Further enhancement was obtained with a second session.
Conclusions: Natural-looking, aesthetically pleasing hair restoration without detectable scars and with reasonable hair density can be obtained in just 1 or 2 sessions through the use of large numbers of follicular micrografts and minigrafts. (Aesthetic Surg J 2003;23:259-264.)
Nordstrom1 and, later, Marrit2 described the use of micrografts (1 or 2 hair grafts) for the frontal hairline to camouflage scars from plugs or previous hair transplantations and to provide a transition zone and a natural-looking front hairline. However, the use of such small grafts was time-consuming and, at the time, appeared impractical for treating large areas of baldness.
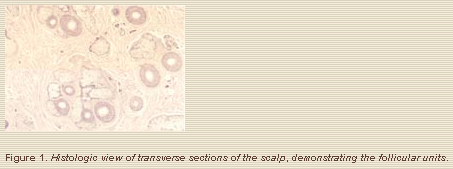
The use of micrografts and minigrafts (3 or 4 hair grafts) in combinations of more than 1000 grafts per session (megasessions) to cover the entire area of baldness was originally described in the mid-1980’s by Uebel.3,4 Headington5 studied the transverse microscopy of the scalp and found that hair grows in follicular units – that is, in groups of 1, 2, 3, or 4 hairs, with each group containing and independent neurovascular bundle, sebaceous glands, sweat glands, and piloerectile muscle, all surrounded by a fine circumferential sheath of collagen. These units appear, to some degree, to be true physiologic entities, so that maintaining them as intact as possible improves hair survival and ultimate hair growth (Figure 1). Skeletonizing the grafts to the bare hair shaft jeopardizes their survival.
Methods
Indications and Contraindications
To be a candidate for this procedure, a patient had to have a favorable ratio of donor hair supply (from the occipital and posterior temporal areas) with respect to the surface area requiring hair restoration. Ideally, he or she was a mature adult, 40 years or older, because at this age the patient’s hair-loss pattern is well established. However, we have also treated younger patients conservatively, as long as they understood that they would continue to lose hair and more than likely would require more additional transplantation procedures. Although the transplanted hair generally is quite durable, the primary or native hair of the patterned area of hair loss will tend to continue shedding.
During the initial consultations, candidates were told that 1 session would give them significant improvement but that a second session is often required to achieve optimal results with regard to hair density. Factors such as thickness (hair mass), color, and texture also affect the final result, especially with respect to the appearance of hair density (fullness).
Individuals with a very limited donor area and large areas of baldness were not candidates for this procedure.
Patients
Between March 1994 and March 2002, 453 consecutive patients, comprising 399 men and 54 women, underwent hair transplantation, performed in accordance with the technique described below. Patients ranged in age from 21 to 72 years (mean 42). Follow-up ranged from 6 months to 8 years.
Technique
The final aesthetic result depends on hairline shape and level, irregularity and some degree of asymmetry in contour, direction of hair growth, and absence of detectable scarring. Because patients have different head sizes and craniofacial proportions, no set formula exists with which to determine the ideal distance between the eyebrows and the anterior hairline. An aesthetic approach must take such differences into account in determining the appropriate hairline level, which ranges between 7 and 10 cm.
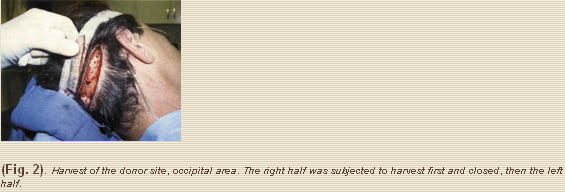
The patient was placed in the supine position, under intravenous sedation with midazolam and fentanyl, and occipital and supraorbital nerve blocks with 0.5% bupivacaine with epinephrine 1:200,000. A horizontal ellipse of scalp was harvested from the occipital area; this sometimes included part of the posterior temporal scalp (Fig. 2). The dimensions of the ellipse varied, depending on the number of grafts planned and the density of the donor site. When 2000 or more grafts were planned, the ellipse generally measured 23 to 26 x 2 cm in width at the midline, tapered to 1.5 cm as it approached about 3 to 5 cm laterally, and beyond that, tapered to 1 cm as it proceded laterally. Scalp tightness was greater laterally than at the midline, and it was important to keep this in mind during closure to avoid undue tension.
I inserted the grafts with the use of a “slit-and-slide” technique, in which the slit was made with a 22.5 Sharpoint blade (Surgical Specialties Corp, Reading, PA) (Fig. 5) and an assistant immediately inserted the graft by sliding it along the side of the blade. To keep grafts from “popping out”, they were initially inserted 5 mm apart. After 20 to 30 minutes, when the fibrinogen had converted to fibrin and the grafts were a bit more stable, I made slits about 2.5 mm apart, again working anteriorly to posteriorly. This process was repeated until all the grafts were inserted ad densely packed, 1 to 1.5 mm apart. Greater emphasis was placed on the anterior scalp rather than the posterior because the anterior is more important in framing the face and the hair can always be combed back to help cover the posterior scalp.
Results
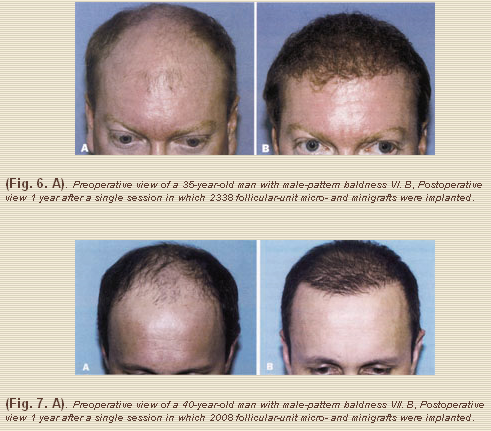
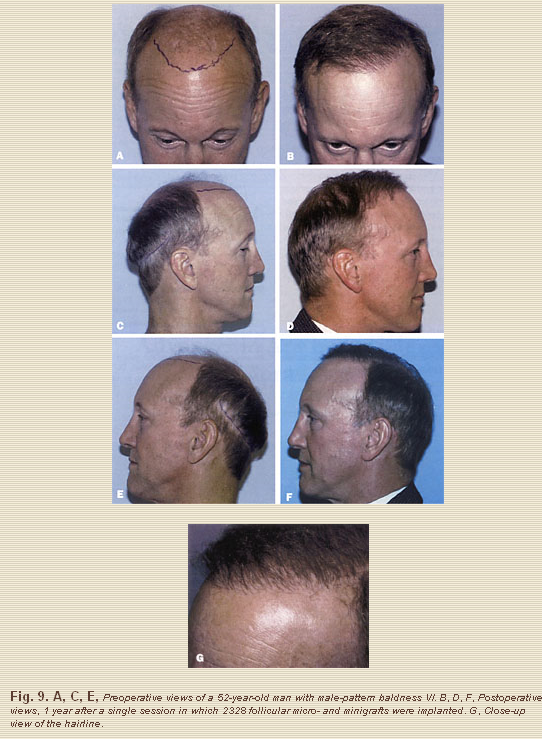
The procedure produced natural-looking in just 1 or 2 sessions, with undetectable scarring (Figures 6-9). Most patient’s older than 50 years were satisfied after a single session. Younger patient’s were more demanding and often requiring a second session before being entirely satisfied with the results. Most of these younger patient’s had always planned to undergo a second procedure.
The following complications occurred in this series of 453 consecutive cases. In 2 patient’s (1 African-American and 1 of Mediterranean origin), keloid scarring developed at the donor site. Two patients experienced poor hair growth. Both cases occurred early in the series, when my assistants were learning to dissect grafts, and these patients were satisfied with their results after a second session. At the time of this writing, we achieve about 95% hair growth from each individual graft. Two cases of alopecia at the donor-site closure developed as a result of ischmia caused by overly tight closures. This complication was revised by excision, grafting, or both.
Discussion
Aesthetic hair restoration cannot restore the hair density patient’s had when they were younger. It can only redistribute the patient’s existing hair in a more strategic way to provide better scalp coverage with a natural-looking hairline. To ensure patient satisfaction, careful selection of patients with an appropriate donor-hair supply and realistic expectations is necessary.
The most difficult aspect of the procedure is achieving sufficient density. With experience, we found that we were able to pack grafts closer to each other, which resulted in improved density in a single session. A second session certainly would further improve the result. Occasionally, I have conducted a third session, enhancing the density even more.
The transplanted hair is quite durable. It is permanent as the hair in the donor area, a most encouraging finding first described as the “donor dominance concept” by Orentreich in 1949.10
Conclusion
Natural and aesthetically pleasing hair restoration, without detectable scars and with reasonable hair density, can be obtained consistently by means of implantation of large numbers (2000-2500) of follicular micrografts and minigrafts in just 1 or 2 sessions.
References
1. Nordstrom REA. Micrografts for improvement of the frontal hairline after hair transplantation. Aesthetic Plast Surg 1981;5:97-106.
2. Marritt E. Single hair transplantation for hairline refinement: a practical solution. J Dermatol Surg Oncol 1984;10:962-966.
3. Uebel CO. Micrografts and minigrafts: a new approach to baldness surgery. Ann Plast Surg 1991;27:479-487.
4. Uebel CO. A new method for pattern baldness surgery. Presented at: Jornada Carioca Cirurgia Plastica; Rio de Janereio, Brazil; August 1986.
5. Headington JT. Transverse microscopic anatomy of the human scalp. Arch Dermatol 1984;120:449-456.
6. Barrera A. Micrograft and minigraft measession hair transplantation: review of 100 consecutive cases. Aesthetic Surg J 1997;17:165-169.
7. Barrera A. Micrograft and minigraft measession hair transplantation results after a single session. Plast Reconstr Surg 1997;100:1524-1530.}
8. Barrera A. Refinements in hair transplantation: micro and minigraft megasession. Perspect Plast Surg 1998;11:53-70.
9. Barrera A. Hair grafting tips and techniques. Perspect Plast Surg 2001;15:147-158.
10. Orentreich N. Autografts in alopecias and other dermatological conditions. Ann N Y Acad Sci 1959;83:463-476.
Alfonso Barrera, M.D.
West Houston Plastic Surgery Clinic, P.A.
915 Gessner Rd., Suite 825
Houston, Texas 77024